What are the complications for Crohn's disease? How they are treated? Read in this article.
Content
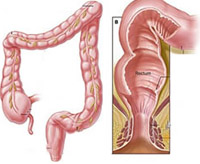
Swistula in Crown Disease
In the clinical picture of Krone's disease, fistulas occupy a prominent place, and in some cases, the disease can only appear in this complication. There are external fistulas with an outlet on the front abdominal wall, internal integrals between the pockets and the hinges adjacent to them, and direct fistulas.
Outer fistula in krone disease
 External fistulas open on the front abdominal wall usually in the scar area remaining after appendectomy or diagnostic laparotomy, and are relatively rare. Appnectomy is preceded by approximately third cases of their development. After surgery produced in connection with suspicion of acute appendicitis, external fistulas arise in 1% of cases.
External fistulas open on the front abdominal wall usually in the scar area remaining after appendectomy or diagnostic laparotomy, and are relatively rare. Appnectomy is preceded by approximately third cases of their development. After surgery produced in connection with suspicion of acute appendicitis, external fistulas arise in 1% of cases.
The mechanism for the development of outer fistulas in the Crown disease is closely related to the penetration of ulcers through all layers of the intestinal wall into the surrounding tissue and the formation of abscess. It is manifested by fever, abdominal pains, in some cases, local tension of the muscles of the front abdominal wall. After spontaneous or operational opening of the abscess, a fistula with purulent separated, sometimes mixed with intestinal content. Swistulas - characteristic complications, above all, lesions, exciting small intestines.
Domestic fistula in crown disease
The mechanism for the formation of internal fistulas is the same as the outdoor. There is a different location of fiscased moves. Most often abscess bursts into the cavity. Therefore, the fools connecting the loops of the ileum are more common, somewhat less often - passing out of the ileum in thick, mainly transverse rim and sigmoid intestine. It occurs and more rare localization of fistula (narrow hole or passage), heading from the ileum in the bladder, ureter, urethra, vagina, uterus, phallopy tube, as well as in a gallbladder and stomach. The clinically of one or another localization of the fistula corresponds to symptoms from the body involved in the pathological process.
The fistulas between the loops of the small intestine lead to the shortening of the intestinal passage (movement) and suction disorders syndrome. At the same time, the fistula of the anorectal region is usually not communicated with the small intestine.
When localizing the Crohn's disease in various departments of the small intestine in 25% of cases, similar changes in the anorectal region can be found at the same time. More often (in 50 - 70% of cases) they are observed in the disease of the Crown, which flows with the defeat of the colon. Sometimes anal changes are the first manifestations of the disease, although it may be the result of greater availability of them for inspection and, therefore, the possibility of diagnosis in the earlier period of the disease.
It described a lot of varieties of the lesion of the anal area during the disease Crown. As a rule, when Crohn's disease, they are wide with subrabate edges of a fissure (gap, furrow), which is located in most cases in the side, and not in the usual rear direction. Sometimes it is a rear or even anterior anal crack. Strong pains are rarely observed, although many patients complain about the unpleasant feelings in the anal area. Crack can be isolated, but sometimes there are two or more. An almost mandatory manifestation of Crohn's disease, accompanied by such fissures, is a significant swelling of perianal tissues. At the same time, the swollen skin around the anus acquires a crimson-blue tint. Crackers are characterized by sluggish and slow regeneration. Due to the strong edema of the mucous membrane and its enhanced folding, these fissors are not always easy to identify. Often they are real longitudinal ulcers, rarely different from ordinary painful anal cracks.
 In more severe cases, the ulcerations achieve such an extent that they affect the entire anal part of the intestine and neighboring areas, up to genital organs. With that, women have reco-vaginal fistulas, abscesses in the bartholine glands and vulvits; Men has a sharp swelling of the scrotum. The process can penetrate into a sedlicate-straightforphic fiber, on the anal muscles and destroy the entire sphincter zone with the formation of an extensive clock in their place. Typical Sounds of the rectum, formed as a result of spontaneous or operational opening of periative and sedanistic-recycled abscesses. Their inner hole can be localized not only near the swollen line, as it usually happens when swashing other etiology, but much proximal. More often there are multiple fistulas with different direction of moves.
In more severe cases, the ulcerations achieve such an extent that they affect the entire anal part of the intestine and neighboring areas, up to genital organs. With that, women have reco-vaginal fistulas, abscesses in the bartholine glands and vulvits; Men has a sharp swelling of the scrotum. The process can penetrate into a sedlicate-straightforphic fiber, on the anal muscles and destroy the entire sphincter zone with the formation of an extensive clock in their place. Typical Sounds of the rectum, formed as a result of spontaneous or operational opening of periative and sedanistic-recycled abscesses. Their inner hole can be localized not only near the swollen line, as it usually happens when swashing other etiology, but much proximal. More often there are multiple fistulas with different direction of moves.
The relatively sluggish flow of fistulas in Crohn's disease. Patients complain of small allocations from the hole of the fistula and the edema of the surrounding skin. Characteristic absence of pain in a long period. Palpation seals along the fistula, as a rule, is not observed.
In the bacteriological study of the detishes separated by the rectum in persons suffering from Crohn's disease, intestinal sticks, protea, strepto- and staphylococcis often find.
Purphoration of intestines during crown disease
In recent years, this is a formidable complication of Crohn's disease, including the breeding of colon. At the same time, with Crohn's disease, perforation into a free abdominal cavity, especially in the small intestine, it rarely happens. The literature describes a little more than one hundred such cases. It is typical of the development of covered perforations, since the inflammatory process with the disease of the Crown usually spreads to all the layers of the intestine walls, including serous (watery, whey) cover.
Serozit (inflammation of serous shells), in turn, contributes to the formation of adhesions with adjacent organs or glands. Therefore, deep sloping ulcers penetrating through the entire thickness of the intestinal wall, lead to the formation of abscesses and fistulas with nearby organs, and not to free perforation. In some cases, the punch of the colon also contributes to the formation of abscesses that can be distributed even on the pelvic bones. Accession to the main disease of acute osteomyelitis changes clinical symptoms; In the lobby of high fever and severe general condition, severe pains and tissue edema arise in the area of affected bones. Sometimes abscess bursts into the hip joint, which leads to septic arthritis.
Diagnostics of perforation in patients, for a long time of treated corticosteroid hormones, which mask signs of this complication. It is believed that the hormones themselves do not lead to the arrangement of the intestinal wall, but due to the weakening of a number of symptoms, first of all, fever and tachycardia are misleading the doctor relative to the presence of this complication. As a result, the danger of delay with operational intervention is created.
The absence of a certain relationship between the duration of the underlying disease and the frequency of development of punching walls of the colon. Sometimes this complication occurs already in the early stage of the process, but often observed in persons, many years suffering from Krone's disease.
Timely diagnosis of this complication is sometimes difficult. The opinions of the authors about the frequency of massive bleeding during the disease of the crown are diverged, since usually the amount of lost blood is estimated on the eye. However, with repeated, even not very abundant blood loss, anemia can develop, quite difficult to treat. Only a small number of patients suddenly occurs such profuse intestinal bleeding, that some measures of conservative treatment is not enough and have to resort to urgent surgery. In these cases, massive bleeding is due to deep ulceration, destroying the walls of large blood vessels.
Acute toxic dilatation of colon with crown disease
Acute toxic dilatation (increasing or expansion) of the colon may occur not only with non-specific ulcerative colitis, but also in the Crohn disease, and refers to the most dangerous complications of this disease.
 Most often, the transverse colon is exposed to acute expansion. In such cases, significant changes usually find, especially in the form of edema, in the field of spleen bend. As a result of the narrowing of the distal part of the transverse colon in the proximal (located nearby), its department accumulates a large amount of gas and liquid fecal masses, which leads to an expansion of the intestine, the walls of which were also amazed by the inflammatory process. Further stretching of the walls of the transverse colon causes degenerative changes in them and ultimately reduce the muscular function. A kind of vicious circle is formed.
Most often, the transverse colon is exposed to acute expansion. In such cases, significant changes usually find, especially in the form of edema, in the field of spleen bend. As a result of the narrowing of the distal part of the transverse colon in the proximal (located nearby), its department accumulates a large amount of gas and liquid fecal masses, which leads to an expansion of the intestine, the walls of which were also amazed by the inflammatory process. Further stretching of the walls of the transverse colon causes degenerative changes in them and ultimately reduce the muscular function. A kind of vicious circle is formed.
The forecast for acute toxic dilatation of the colon is very serious. At all stages of development of complications, there is a threat to the occurrence of perforations of a sharply modified wall of the colon. Perforation for toxic dilatation of the colon can be masked by a severe common state of patients.
For timely diagnosis of this complication, X-ray control should be carried out (abdominal reproducible radiographs). Patients with acute toxic dilatation of colon must be under constant medical supervision. In the absence of the effect of conservative therapy or suspected perforation, urgent surgery is shown. Although the acute expansion is more often observed by the transverse colon, perforation can be localized in other parts of the intestinal tract, for example in a sigmoid intestine.
Frequent and serious complications of Crohn's disease include strictures, t. E. Resistant narrowings of fine, colon and rectum. Strictures can be single or multiple, and in the latter cases are divided into more or less extensive areas of the normal mucous membrane.
For a long time of narrowing in the disease Crown, the asymptomatic and passage of intestinal content occurs, it is unhindered, apparently due to the compensatory hypertrophy of the muscular layers of the walls located above the colon departments. However, the symptoms of chronic intestinal obstruction may eventually appear, especially when localizing strictures in the terminal department of the ileum. Strong gravating pain in the stomach, vomiting, stool delay and gases appear. Along with the swelling of the intestine, percussionly conditioning high tympanite, becomes visible to their peristalism. X-ray study at the same time reveals horizontal liquid levels in the intestines (bowls).
Extract inflammatory strictures from strictures formed in connection with malignant gut tumors, quite difficult. When localizing strictures in the rectum, they can sometimes be differentiated using a finger research. In cases of inflammatory origin of the stricture is less dense and, overcoming some resistance, it is usually possible to introduce a finger into the rectum. However, in some cases, they are so hard that only histological examination of the tissue makes it possible to eliminate the rectum cancer.
If the stricture is localized in the colon, then the difference between its benign and malignant nature can be installed only with a radiographic study. In terms of cases, to eliminate the colon cancer, it is necessary to produce laparotomy and biopsy of the affected area.